
From the 1Department of Orthopaedics, and 2Department of Cardiology, The People’s Hospital of Bishan District, Bishan, Chongqing, China
#These authors contributed equally to this work and should be considered co-first authors.
Background: Home-based rehabilitation following hip fracture may be beneficial; however, the evidence is controversial. The aim of this systematic review and meta-analysis was to evaluate the effectiveness of home-based rehabilitation in patients with hip fracture.
Methods: PubMed, Embase, Web of Science, EBSCO, and Cochrane Library databases were searched systematically. Randomized controlled trials (RCTs) assessing the effect of home-based rehabilitation for patients with hip fracture were included. Two investigators independently searched articles, extracted data, and assessed the quality of included studies. Primary outcomes were mobility and daily activity. Meta-analysis was performed using the random-effect model.
Results: Nine RCTs involving 887 patients were included in the meta-analysis. Overall, compared with control intervention for hip fracture, home-based rehabilitation was found to significantly improve mobility (standard mean difference (SMD) 0.56; 95% confidence interval (95% CI) 0.24–0.87; p = 0.006), daily activity (SMD 0.72; 95% CI 0.12–1.33; p = 0.02), instrumental activity (SMD 0.85; 95% CI 0.06–1.64; p = 0.03) and balance (SMD 0.89; 95% CI 0.06–1.73; p = 0.04), but resulted in no significant influence on walking outdoors (risk ratio (RR) 1.36; 95% CI 0.74–2.49; p = 0.32), usual gait speed (SMD 0.28; 95% CI –0.33 to 0.90; p = 0.37), fast gait speed (SMD 0.34; 95% CI –0.54 to 1.22; p = 0.45), and emergency department visit (RR 0.69; 95% CI 0.11–4.32; p = 0.69).
Conclusion: The results of the meta-analysis showed that home-based rehabilitation has considerable positive effects on physical functioning after hip fracture. Home-based rehabilitation is therefore recommended for hip fracture.
Key words: home-based rehabilitation; hip fracture; mobility; daily activity; meta-analysis.
Accepted Jan 24, 2018; Epub ahead of print May 21, 2018
J Rehabil Med 2018; 50: 481–486
Correspondence address: Shaowei Zhang. Department of Orthopedics, The People’s Hospital of Bishan District, Bishan, Chongqing 402760, P.R. China. E-mail: 408887507@qq.com
Home-based rehabilitation following hip fracture may be beneficial. A systematic review and meta-analysis was carried out to evaluate the effectiveness of home-based rehabilitation in patients with hip fracture. Nine RCTs involving 887 patients were included in the meta-analysis. Home-based rehabilitation showed considerable positive effects on physical function after hip fracture. Home-based rehabilitation is therefore recommended for hip fracture. Home-based rehabilitation following hip fracture may be beneficial. A systematic review and meta-analysis was carried out to evaluate the effectiveness of home-based rehabilitation in patients with hip fracture. Nine RCTs involving 887 patients were included in the meta-analysis. Home-based rehabilitation showed considerable positive effects on physical function after hip fracture. Home-based rehabilitation is therefore recommended for hip fracture.
Hip fracture is a major trauma, which results in low physical activity in older people during the inpatient period and for a long time thereafter (1–3). After a hip fracture, many elderly people never regain their pre-fracture levels of mobility and activity, leading to substantial changes in their life, with long-term personal and social consequences (4, 5). There is a high rate of cognitive impairment (e.g. dementia) among older people with hip fractures (6). Physical activity and organized rehabilitation are crucial to prevent further falls, disability and several chronic diseases (7, 8). In addition, physical activity has positive short-term effects on health and mobility recovery after injury or surgery (9, 10).
More attention should be given to extended rehabilitation programmes to improve mobility and physical activity after hip fracture (11, 12). Home-based rehabilitation programmes are designed for patients who cannot attend supervised training sessions outside the home and may also be suitable for frail patients with hip fracture. Such programmes mainly include physical exercise, safety assessment, and self-efficacy based motivational component (13). Supervised home-based training programmes have been shown to increase the amount of time spent on exercise activities and activity level in patients with hip fracture (14, 15). One 12-month individualized home rehabilitation programme was reported to increase physical activity among older patients with hip fracture and demonstrate long-term efficacy (16).
In contrast to these studies, however, some relevant RCTs have shown that a home-based rehabilitation programme had no substantial influence on daily activity, instrumental activity, walking outdoors and gait speed in patients treated for hip fracture (17–19). Considering these inconsistent results, we therefore conducted a systematic review and meta-analysis of RCTs to evaluate the effectiveness of home-based rehabilitation in patients with hip fracture.
This systematic review and meta-analysis was conducted according to the guidance of the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement (20) and the Cochrane Handbook for Systematic Reviews of Interventions (21). All analyses were based on previous published studies, thus ethical approval and patient consent were not required.
PubMed, Embase, Web of Science, EBSCO, and the Cochrane Library were systematically searched from January 1980 to September 2017, with the following keywords: home, and rehabilitation or exercise, and hip fracture. To include additional eligible studies, the reference lists of retrieved studies and relevant reviews were also hand-searched and the process above was performed repeatedly until no further article was identified.
The inclusion criteria were as follows: study population, patients with hip fracture; intervention, home-based rehabilitation; control, usual care; outcome measure, mobility, daily activity; and study design, RCT.
The following information was extracted for the included RCTs: first author, publication year, sample size, baseline characteristics of patients, home-based rehabilitation, control, study design, mobility, daily activity, instrumental activity, balance test, walking outdoors, usual gait speed, fast gait speed, emergency department visit. If necessary the author was contacted to acquire the data.
Primary outcomes were mobility and daily activity. Secondary outcomes included instrumental activity, balance test, walking outdoors, usual gait speed, fast gait speed, emergency department visit.
The Jadad Scale was used to evaluate the methodological quality of each RCT included in this meta-analysis (22). This scale consists of 3 evaluation elements: randomization (0–2 points), blinding (0–2 points), dropouts and withdrawals (0–1 points). One point was allocated to each element if it was mentioned in the article, and another point was given if the methods of randomization and/or blinding had been described appropriately and in detail. If methods of randomization and/or blinding were inappropriate, or dropouts and withdrawals had not been recorded, then 1 point was deducted. The Jadad Scale score varied from 0 to 5 points. An article with Jadad score ≤ 2 was considered to be of low quality. If the Jadad score ≥ 3, the study was considered to be of high quality (23).
Standard mean differences (SMD) with 95% confidence intervals (95% CIs) for continuous outcomes (mobility, daily activity, instrumental activity, balance test, usual gait speed, fast gait speed), and risk ratios (RRs) with 95% CIs for dichotomous outcomes (walking outdoors, emergency department visit) were used to estimate the pooled effects. All meta-analyses were performed using the random-effects model with DerSimonian and Laird weights. Heterogeneity was tested using the Cochran Q statistic (p < 0.1) and quantified with the I2 statistic, which described the variation of effect size that was attributable to heterogeneity across studies. An I2 value greater than 50% indicated significant heterogeneity. Sensitivity analysis was performed to detect the influence of a single study on the overall estimate via omitting one study in turn when necessary. Publication bias was not assessed because there was a limited number of included studies (n = 9). A p < 0.05 in 2-tailed tests was considered statistically significant. All statistical analyses were performed with Review Manager Version 5.3 (The Cochrane Collaboration, Software Update, Oxford, UK).
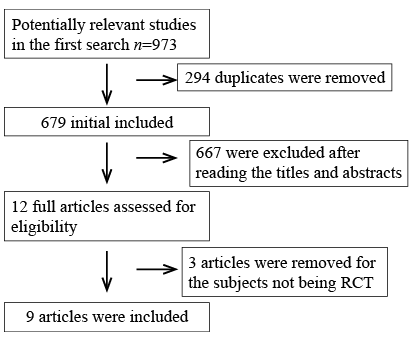
The flow chart for the selection process and detailed identification is shown in Fig. 1. A total of 973 publications were identified through the initial search of databases. Of these, 294 duplicates were removed, 667 studies were excluded (due to irrelevant subject matter) on the basis of initial screening of the titles and abstracts. And 3 papers were removed for the subjects not being RCTs. Ultimately, 9 RCTs were included in the meta-analysis (13, 15–19, 24–26).
Fig. 1. Flow diagram of study searching and selection process.
The baseline characteristics of the 9 eligible RCTs in the meta-analysis are summarized in Table I. The 9 studies were published between 2008 and 2017, and sample sizes ranged from 26 to 232 with a total of 887. In all studies, there were similar age, body mass index (BMI), proportion of women/men, and of participants living alone between home rehabilitation group and control group at baseline. Two studies involved the same samples at different follow-up time by Turunen & Salpakoski (16, 24), and Ziden et al. (25, 26).
Among the 9 RCTs, 2 studies reported mobility (13, 26), 4 reported daily activity (13, 17, 19, 25), 3 reported instrumental activity (17, 25, 26), 2 reported balance test (13, 26), 2 reported walking outdoors (18, 26), 2 reported usual gait speed (18, 19), 2 reported fast gait speed (18, 19), and 2 reported emergency department visit (15, 24). Jadad scores of the 9 included studies varied from 3 to 5, and all studies were considered to be high-quality according to quality assessment.
Table I. Characteristics of included studies
The outcome data were analysed with a random-effects model, the pooled estimate of the 2 included RCTs suggested that, compared with control group for hip fracture, home-based rehabilitation was associated with significantly increased mobility (SMD 0.56; 95% CI 0.24–0.87; p = 0.006), with low heterogeneity among the studies (I2 = 0%, heterogeneity p = 0.18, Fig. 2A).
Home-based rehabilitation consistently resulted in substantially improved daily activity for hip fracture (SMD 0.72; 95% CI 0.12–1.33; p = 0.02) with significant heterogeneity among the studies (I2 = 86%, heterogeneity p < 0.0001, Fig. 2B).
Fig. 2. Forest plot for the meta-analysis of (A) mobility, (B) daily activity, (C) instrumental activity, (D) balance test, (E) walking outdoors, (F) usual gait speed (m/s), (G) fast gait speed (m/s), and (H) emergency department visit.
Low heterogeneity of mobility and significant heterogeneity of daily activity were observed among the included studies. However, there was still significant heterogeneity for daily activity after performing sensitivity analysis by omitting one study in turn in order to detect the source of heterogeneity.
Compared with control intervention for hip fracture, home-based rehabilitation showed significantly improved instrumental activity (SMD 0.85; 95% CI 0.06–1.64; p = 0.03; Fig. 2C) and balance test (SMD 0.89; 95% CI 0.06–1.73; p = 0.04; Fig. 2D), but had no substantial impact on walking outdoors (RR 1.36; 95% CI 0.74–2.49; p = 0.32; Fig. 2E), usual gait speed (SMD 0.28; 95% CI –0.33 to 0.90; p = 0.37; Fig. 2F), fast gait speed (SMD 0.34; 95% CI –0.54 to 1.22; p = 0.45; Fig. 2G), or emergency department visit (RR 0.69; 95% CI 0.11–4.32; p = 0.69; Fig. 2H).
Home-based rehabilitation for older people with hip fractures has been reported to have better long-term results in terms of walking ability than living in ordinary housing (16, 27). The current meta-analysis suggests that home-based rehabilitation is associated with significantly improved mobility, daily activity, instrumental activity and balance after hip fracture.
However, no statistical difference was found regarding walking outdoors, usual gait speed, fast gait speed, and emergency department visit between home-based rehabilitation and control based on the results of the current meta-analysis. Participants with poor physical function have been reported not to benefit from home-based rehabilitation programmes (18). A possible explanation for this is that participants with poor physical function already have muscle weakness and mobility impairment prior to the hip fracture. They may not have sufficient capacity to perform home-based exercises or to go outdoors independently for out-of-home physical activities. For instance, older people with dementia would normally receive shorter duration of rehabilitation following hip fracture, and thus show less improvement in walking ability (18, 28, 29). Previous walking ability and the presence of complications (e.g. delirium or pressure ulcers) can determine functional recovery more than cognitive impairment does (30). More supervision and care is needed to improve the efficacy of home-based rehabilitation for patients with hip fracture (16).
Regarding sensitivity analysis, we found low heterogeneity of mobility and significant heterogeneity of daily activity. Significant heterogeneity still remained for daily activity when performing sensitivity analysis by omitting one study in each turn. The possible explanations include different duration, frequency, and intensity of home-based rehabilitation, as well as different physical function before hip fracture.
Previous studies demonstrated that patients with hip fracture undergoing comprehensive rehabilitation were more physically active and had better mobility and physical function several months after surgery (31, 32). The comprehensive geriatric assessment and intervention was revealed to have a positive effect on mobility, especially among older people with hip fracture (33, 34). The optimal duration, frequency, and intensity of home-based rehabilitation interventions after hip fracture remains unclear, and is very important to achieve improvements in physical function (35). Home-based rehabilitation has been shown to require few home visits, but to lead to significant improvements in independence, balance confidence, and physical activity (18, 26, 36). Possible factors for this are that study participants lived in ordinary housing and had no severe cognitive impairment, and they could have had the ability to exercise on their own.
Several limitations should be taken into account. Firstly, 4 of the included RCTs have a relatively small sample size (n < 100). Overestimation of the treatment effect is more likely in smaller trials compared with larger samples. There is significant heterogeneity, possibly due to different duration, frequency, and intensity of home-based rehabilitation, as well as different physical function before hip fracture. The follow-up time ranges from 1 to 24 months, which may affect the pooling results. Finally, some missing data might have led to bias concerning the pooled effect.
In conclusion, this meta-analysis showed that home-based rehabilitation has considerable positive effects on physical functioning after hip fracture. Home-based rehabilitation is therefore recommended for patients after hip fracture.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize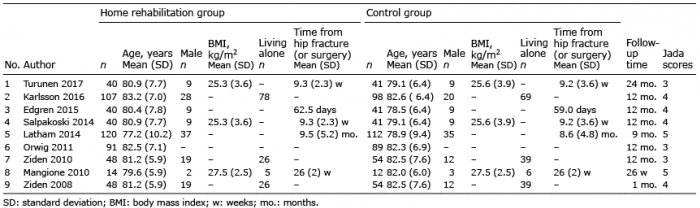 Click to show fullsize
Click to show fullsize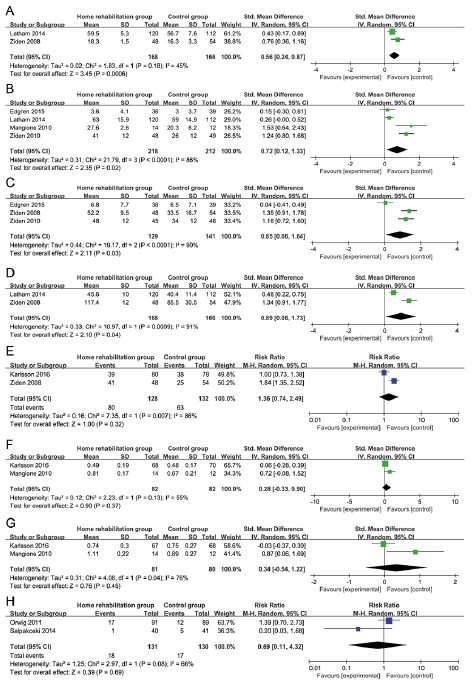 Click to show fullsize
Click to show fullsize